TARGET DECK: MED::I::Signaling Pathways in Health and Disease::Metabolic Biochemistry::04 - Overview of Carbohydrate Metabolism
Topics Covered
- Digestion and absorption
- General scheme: role of liver and extra-hepatic tissues
- Glycogen synthesis and breakdown
- Glycolysis
- Pyruvate oxidation
- Tricarboxylic Acid (TCA) Cycle
- Gluconeogenesis
- Pentose phosphate shunt
The Big Picture
Before diving in, keep this mental model in mind: the body needs a continuous supply of glucose, but you only eat occasionally. The entire system below — digestion, transport, hormonal signalling, and enzymatic control — exists to solve that single problem.
The journey of carbohydrates follows this arc:
- Eat → dietary carbs are digested into monosaccharides
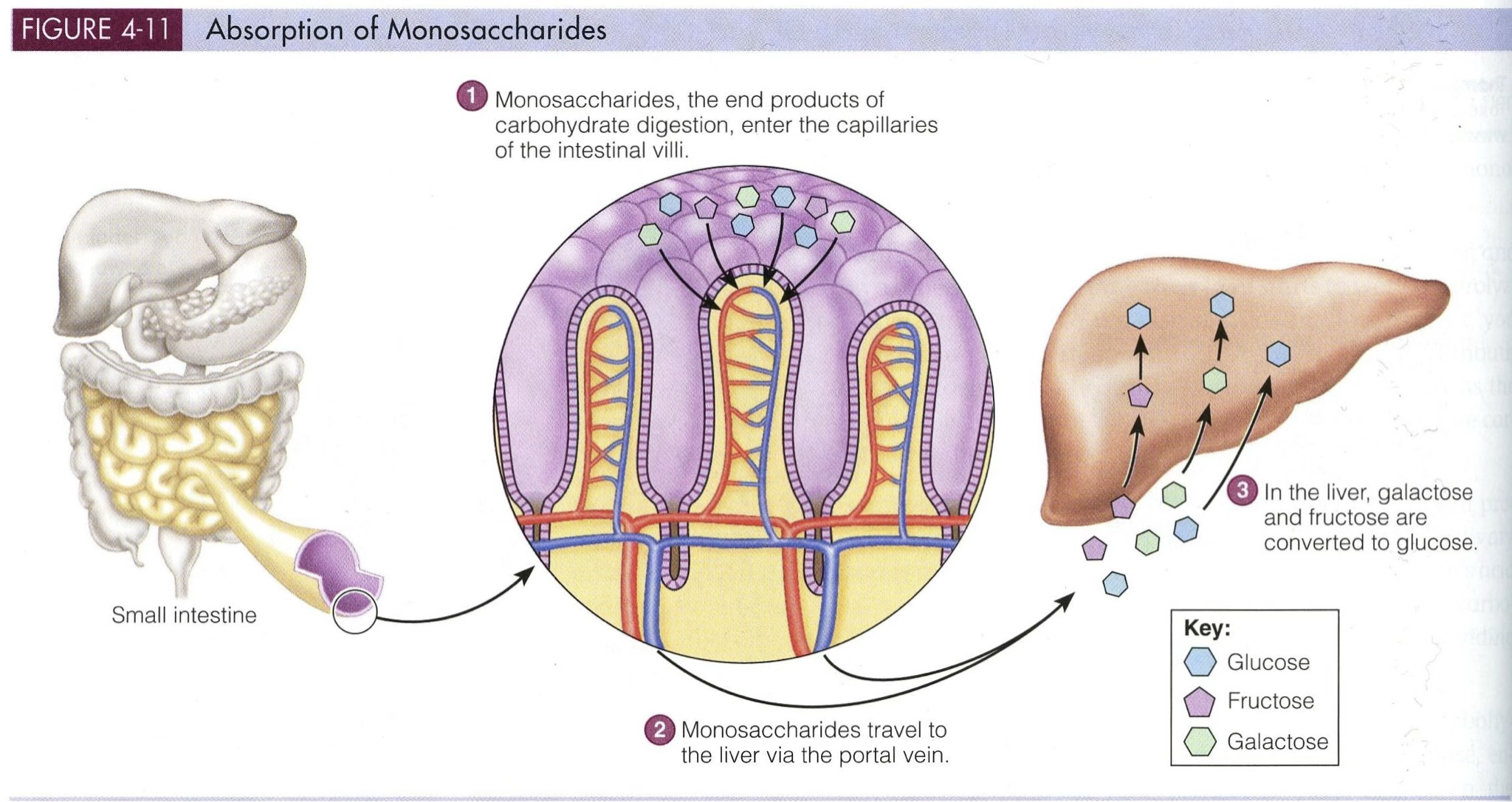
- Absorb → monosaccharides cross the intestinal wall into portal blood
- Distribute → the liver acts as a gatekeeper, deciding what to store vs. release
- Regulate → insulin and glucagon continuously adjust the balance based on nutritional state
Step 1 — Digestion and Intestinal Absorption
What We Eat
The three major dietary carbohydrates are:
| Molecule | SMILES |
|---|---|
| Glucose | $smiles=C([C@@H]1[C@H]([C@@H]([C@H](C(O1)O)O)O)O)O |
| Fructose | $smiles=OC[C@@H]1OC(O)(CO)[C@@H](O)[C@@H]1O |
| Glycogen | Branched polymer of α-D-glucose (α-1,4 and α-1,6 linkages) |
| Starch | Linear (amylose) and branched (amylopectin) α-D-glucose polymer |
Polysaccharides and disaccharides can’t be absorbed directly — they must first be broken down:
| Carbohydrate | Type | Products |
|---|---|---|
| Starch | Polysaccharide | Glucose |
| Lactose | Disaccharide | Galactose + Glucose |
| Sucrose | Disaccharide | Fructose + Glucose |
- Digestion: Amylases from saliva and pancreas cleave starch
- Absorption: Monosaccharides cross intestinal microvilli via secondary active transport
Step 2 — How Glucose Crosses the Intestinal Wall
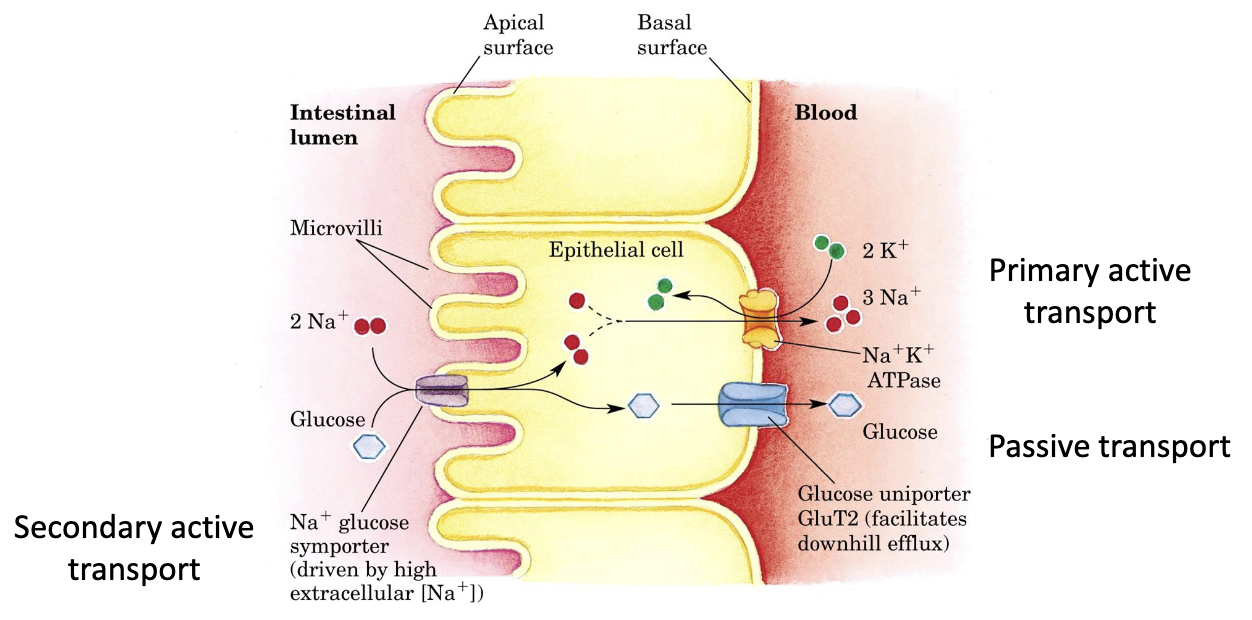
The core problem: glucose needs to move uphill (against its concentration gradient) from the intestinal lumen into the enterocyte. The body solves this by coupling glucose movement to Na⁺ moving downhill.
Energetics of Intestinal Co-transport
Transport Steps (Apical → Basolateral)
- Secondary active transport → Glucose + 2 Na⁺ enter the enterocyte together via SGLT1
- Primary active transport → Na⁺/K⁺-ATPase pumps Na⁺ back out, maintaining the gradient
- Passive transport → Glucose exits down its concentration gradient via GLUT2 into portal blood
How is glucose absorbed from the intestine?
Glucose enters enterocytes by secondary active transport with Na⁺ via SGLT1, then exits to portal blood via GLUT2.
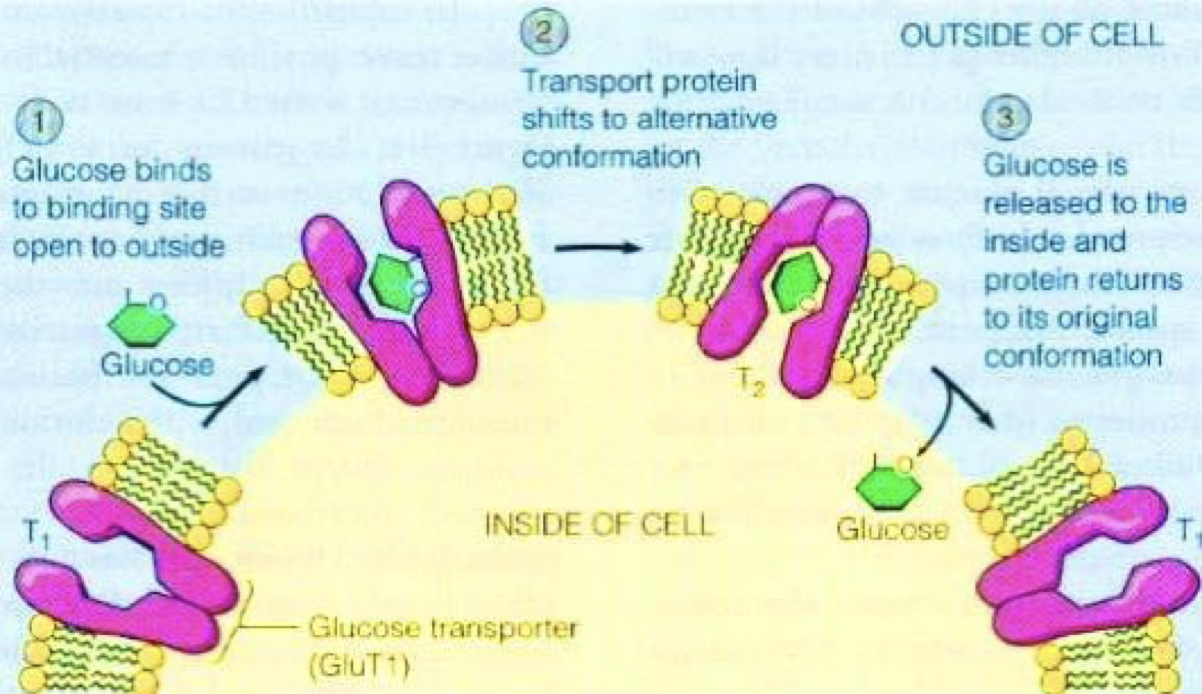
Step 3 — Glucose in the Blood: GLUT Transporters
Once in the portal blood, glucose reaches tissues via GLUT transporters. Different tissues express different GLUTs — this is not arbitrary. Each isoform is tuned to the physiological needs of that tissue.
| GLUT | Location | Features | (substrate) mM |
|---|---|---|---|
| GLUT1 | Ubiquitous (RBCs, brain) | High affinity, basal uptake | 5 (glucose) |
| GLUT2 | Liver, pancreatic β-cells, intestine | Low affinity, high capacity | 10-15 (glucose, [galactose & fructose]) |
| GLUT3 | Neurons | Very high affinity | 1-2 (glucose) |
| GLUT4 | Muscle, adipose tissue | Insulin-dependent | 3-5 (glucose) |
| GLUT5 | Small intestine, sperm | Fructose transporter | 6 (fructose) |
Why does GLUT2 have such low affinity?
The liver only needs to take up large amounts of glucose when blood glucose is already high (postprandially). Low affinity = the liver acts as a buffer, not a competitor.
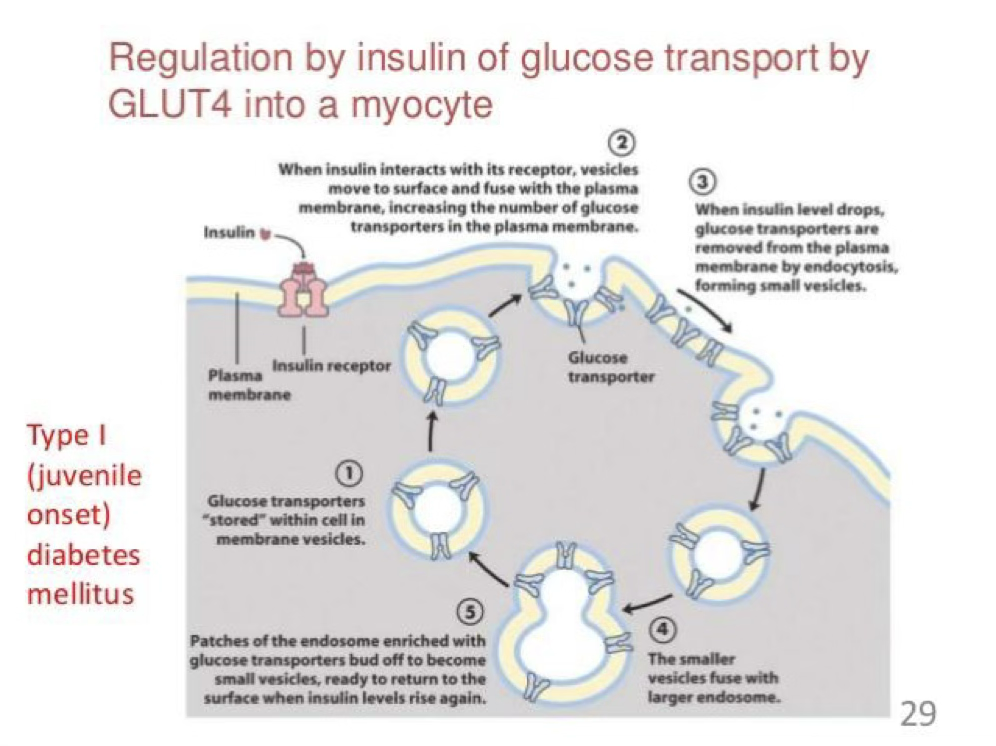
GLUT4 and Insulin
GLUT4 can be regulated by insulin.
Which GLUT transporter is insulin-dependent?
GLUT4 in muscle and adipose tissue.
- Storage (The “Waiting Room”)
Normally, GLUT4 transporters aren’t on the cell’s surface. They are tucked away inside the cell in small bubbles called vesicles. They are basically “off-duty” and waiting for a signal.
- The Insulin Signal (The “Green Light”)
When you eat, your pancreas releases insulin.
- Binding: Insulin binds to an insulin receptor on the cell membrane (the pink structure in your image).
- Translocation: This sends a signal that tells the GLUT4 vesicles to move toward the surface and fuse with the plasma membrane.
- Action: Now that the “doors” are open on the surface, glucose can flood into the cell to be used for energy.
- Removal (The “Closing Time”)
Once your blood sugar levels drop, insulin levels also decrease.
- Endocytosis: The cell pinches the membrane back inward, swallowing the GLUT4 transporters.
- Recycling: These transporters are pulled back into the cell, forming new vesicles (Steps 4 and 5) where they stay until the next meal.
Anatomical Route of Absorbed Glucose
Glucose enters hepatocytes postprandially via GLUT2 at the hepatic sinusoids.
Glycaemic Regulation
A glycaemic peak follows a carbohydrate-rich meal. Regulation is primarily mediated by insulin (↑ uptake) and glucagon (↑ production).
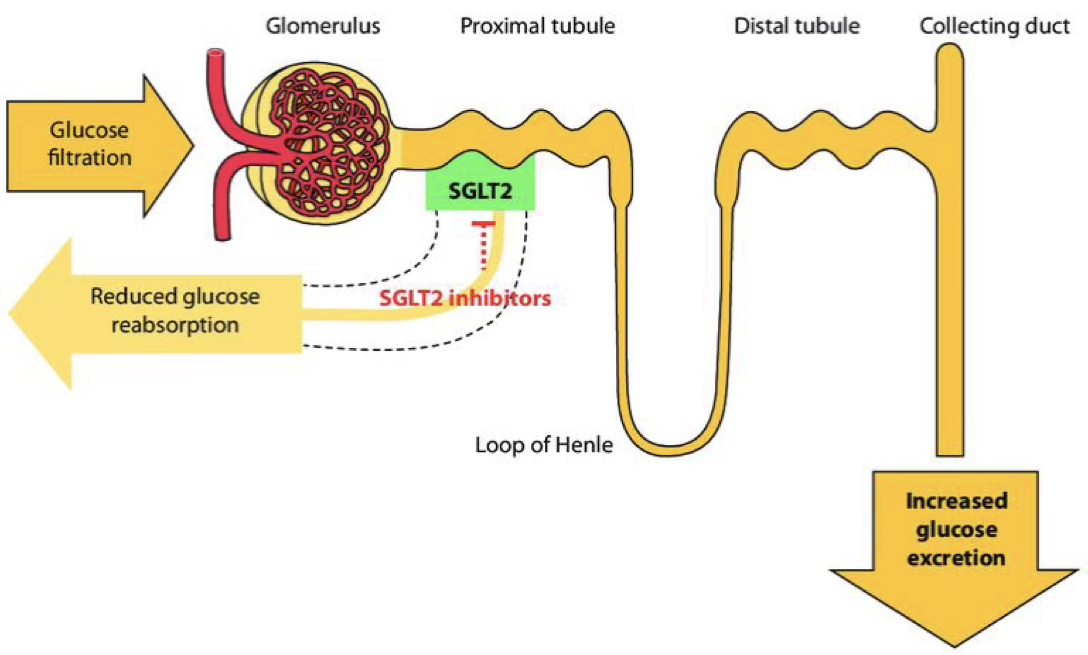
Step 4 — Renal Handling of Glucose
The kidney filters glucose continuously. Under normal conditions, all of it is reclaimed — glucosuria is a sign that the system is overwhelmed.
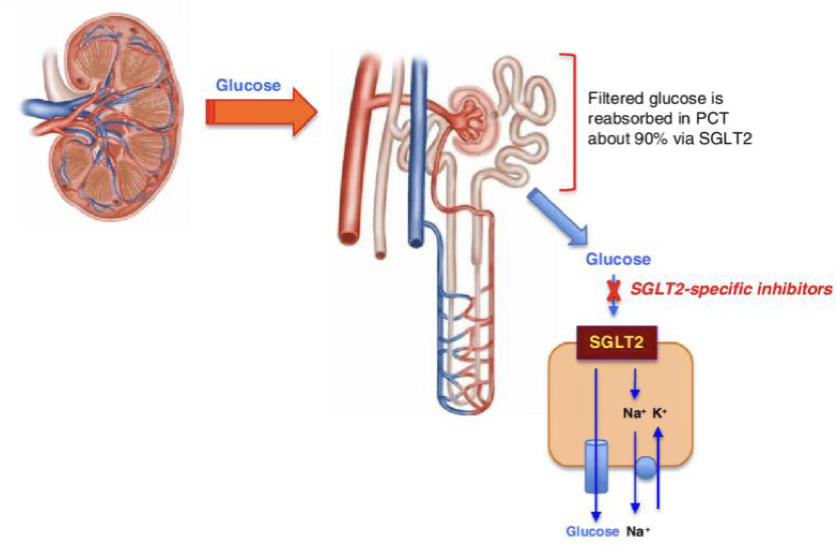
Reabsorption: Where and How
| Segment | Transporter | Affinity | Capacity | % Glucose Reabsorbed |
|---|---|---|---|---|
| Early PCT | SGLT2 | Low | High | ~90% |
| Late PCT | SGLT1 | High | Low | ~10% |
- Basolateral exit into the bloodstream: via GLUT2 and GLUT1
- Driving force: Na⁺/K⁺-ATPase maintains the electrochemical gradient for SGLT activity
Renal Threshold for Glucose (RTG)
Renal Glucose Threshold
In healthy individuals, the RTG is approximately 180–200 mg/dL. Below this concentration, virtually all filtered glucose is reabsorbed. Above it, glucose appears in the urine (glucosuria).
What is the renal threshold for glucose in healthy individuals?
About 180–200 mg/dL; above this, glucose appears in urine.
Transport Maximum (Tm) — the ceiling on reabsorption capacity:
RTG varies with physiological state:
| Condition | RTG |
|---|---|
| Healthy adult | 180–200 mg/dL |
| Pregnancy / Children | < 126 mg/dL |
| Type 2 Diabetes | 200–250 mg/dL |
Step 5 — Hormonal Control: Insulin vs. Glucagon
This is the master switch. Everything downstream — glycolysis, gluconeogenesis, glycogen metabolism — is tuned by the insulin:glucagon ratio.
| Hormone | Pathways Activated | Net Effect |
|---|---|---|
| Insulin | Glycogen synthesis, Glycolysis, Pentose phosphate pathway, Lipid synthesis | ↓ Blood glucose |
| Glucagon | Glycogenolysis, Gluconeogenesis | ↑ Blood glucose |
What is the main metabolic effect of insulin versus glucagon?
Insulin promotes glycogen synthesis, glycolysis, PPP, and lipid synthesis; glucagon promotes glycogenolysis and gluconeogenesis.
Postprandial State (Insulin Active)
You just ate. Blood glucose is high. The goal: store and use.
Glucose → Glucose-6-P → Glycogen (liver & muscle)
→ Glycolysis → Pyruvate → CO₂ + H₂O (+ ATP)
→ Lipid synthesis
Fasting State (Glucagon Active – Liver)
Hours since last meal. Blood glucose is falling. The goal: maintain supply.
Glycogen → Glycogenolysis → Glucose-6-P → Glucose (→ blood)
Amino acids → Gluconeogenesis → Glucose-6-P → Glucose (→ blood)
Skeletal Muscle (No Glucagon Receptors)
Why does muscle not respond to glucagon?
Muscle cannot release glucose into the blood (it lacks glucose-6-phosphatase). Allowing glucagon to mobilise muscle glycogen would be useless for maintaining blood glucose — so the receptor is simply absent.
Blood Glucose → (Insulin ↑) → Glucose-6-P
→ Glycogen
→ 2 Pyruvate → CO₂ + H₂O (25 ATP)
→ Lactate (→ blood)
Net: 2 ATP (substrate level) + 25 ATP (oxidative) per glucose
Step 6 — Trapping Glucose: Phosphorylation
Once glucose enters a cell, the first priority is to trap it so it can’t diffuse back out. This is done by phosphorylating it to Glucose-6-Phosphate (G6P).
The Enzymes
The reverse reaction — releasing free glucose — requires a different enzyme:
Futile Cycle
Running both reactions simultaneously wastes ATP with no net result:
This is prevented by hormonal regulation (see table below).
Why is the glucose/glucose-6-phosphatase pair considered a futile cycle?
Because running both reactions at once wastes ATP without changing the glucose pool.
Hormonal Transcriptional Control
| Enzyme | Induced by | Inhibited by | Effect on Glycaemia |
|---|---|---|---|
| Glucokinase | Insulin | Glucagon | ↓ |
| Glucose-6-Phosphatase | Glucagon | Insulin | ↑ |
Hexokinase vs. Glucokinase — Why Two Enzymes?
Both phosphorylate glucose, but they serve different masters:
| Property | Glucokinase (GK) | Hexokinase (HK) |
|---|---|---|
| Location | Liver, pancreatic β-cells | All other tissues |
| Affinity | Low (high Km) | High (low Km) |
| Substrate specificity | Glucose only | Glucose, fructose, mannose |
| Product inhibition | Not inhibited by G6P | Inhibited by G6P |
| Insulin induction | Yes | No |
| Kinetics | Sigmoidal (cooperative) | Hyperbolic (Michaelis-Menten) |
The logic:
Hexokinase works in all tissues and is always active at physiological glucose concentrations (high affinity).
Glucokinase is a liver-specific glucose sensor — it only becomes active when glucose is abundant, and it never saturates, so the liver keeps removing glucose proportional to how high blood sugar climbs.
Glucokinase Regulatory Protein (GKRP) — Fine-Tuning in the Liver
- Fasting: GKRP sequesters GCK in the nucleus → GCK is inactive
- Postprandial (high glucose): GCK is released into the cytoplasm → phosphorylates glucose → supports glycogen synthesis
- F6P stabilises the GCK–GKRP complex → enhanced inhibition (fasting signal)
- F1P disrupts the complex → releases active GCK (fed signal, from fructose metabolism)
What Happens to G6P?
All three downstream pathways are stimulated by insulin and inhibited by glucagon:
Glucose-6-P ──→ Glycogen synthesis (storage)
──→ Glycolysis (energy)
──→ Pentose phosphate pathway (biosynthesis & antioxidant defence)
Appendix — Kinase/Phosphatase Primer
Kinase = phosphotransferase:
Note
In protein kinases, X is a Ser, Thr, or Tyr residue. Many kinase reactions are irreversible; the reverse is catalysed by a phosphatase:
TLDR - 04 - Overview of Carbohydrate Metabolism
TLDR – Overview of Carbohydrate Metabolism
Digestion & Absorption:
Dietary carbohydrates (starch, lactose, sucrose) are broken down by salivary and pancreatic amylases into monosaccharides (glucose, fructose, galactose). These are absorbed in the intestine via secondary active transport (SGLT1, driven by the Na⁺ gradient maintained by Na⁺/K⁺-ATPase) and exit into the portal blood via GLUT2.Glucose Transport:
GLUT transporters mediate tissue-specific glucose uptake. GLUT4 in muscle and adipose tissue is insulin-dependent. GLUT2 in the liver acts as a glucose sensor (low affinity, high capacity).Renal Handling:
The kidney reabsorbs ~90% of filtered glucose via SGLT2 (early PCT) and ~10% via SGLT1 (late PCT). The renal threshold is ~180–200 mg/dL; above this, glucosuria occurs. Tm is 375 mg/min (men) and 300 mg/min (women).Insulin vs. Glucagon:
- Insulin (postprandial): activates glycogen synthesis, glycolysis, pentose phosphate pathway, and lipid synthesis → lowers blood glucose
- Glucagon (fasting): activates glycogenolysis and gluconeogenesis → raises blood glucose
- Skeletal muscle has no glucagon receptors; glucose metabolism there is primarily insulin-driven
Glucose Phosphorylation:
Glucose is trapped in cells as Glucose-6-Phosphate by hexokinase (all tissues, high affinity, inhibited by G6P) or glucokinase (liver/pancreas, low affinity, not inhibited by G6P, insulin-induced). G6P can be released back to glucose only in liver and kidney (glucose-6-phosphatase). Running both enzymes simultaneously creates a futile cycle, prevented hormonally.GKRP sequesters glucokinase in the nucleus during fasting; high glucose and F1P release it into the cytosol, while F6P enhances its nuclear retention.
G6P fates (all insulin-stimulated, glucagon-inhibited): glycogen synthesis, glycolysis, pentose phosphate pathway.